Posts Tagged ‘community organisations’
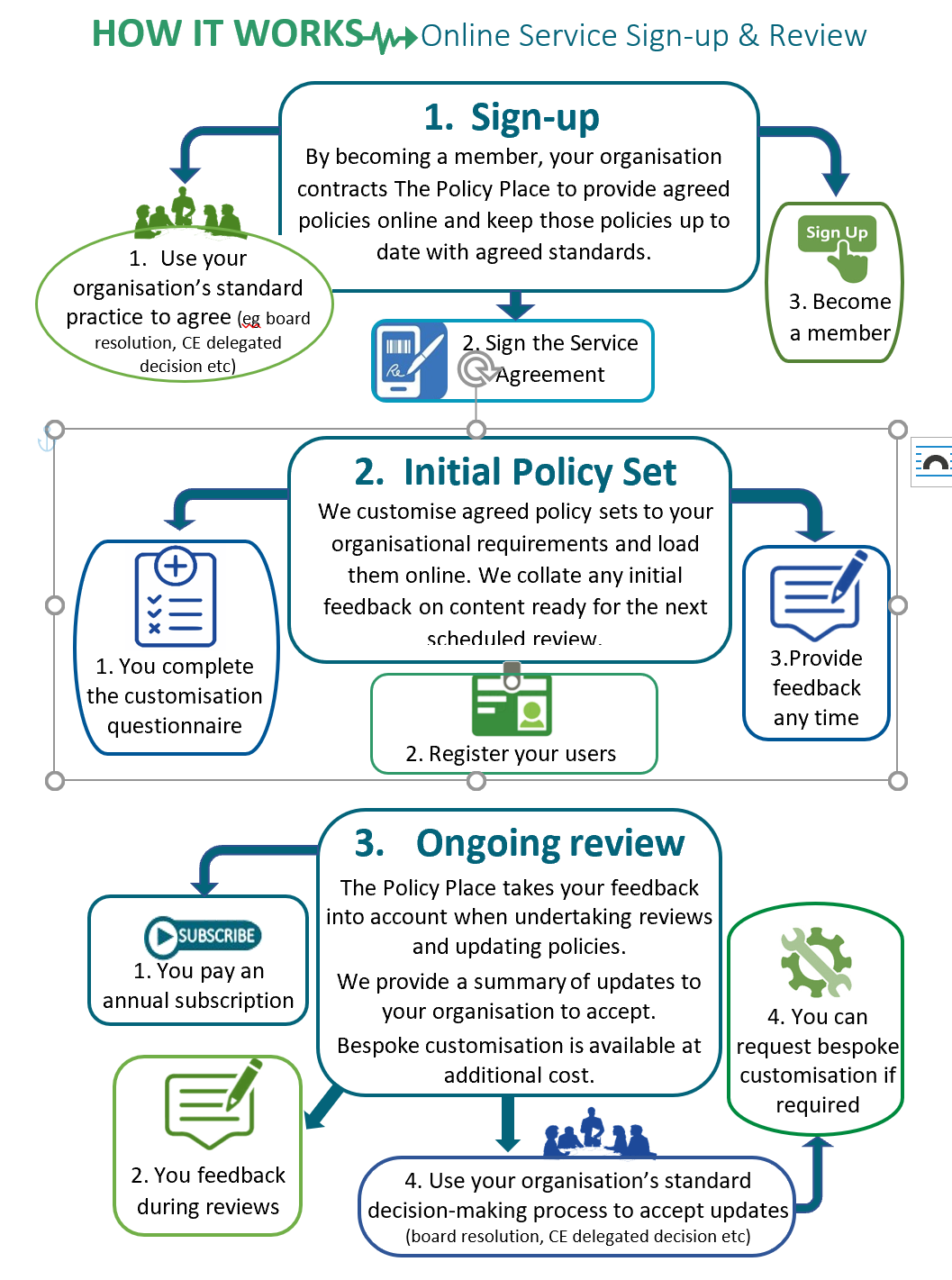
Online policies and procedures – so easy!

Get that makimaki/monkey off your back
There’s been a lot of change in law, policy and practice recently affecting social, health and disability services. There is likely to be more.
In this post, we overview some key changes to consider when reviewing and updating your organisation’s policies and procedures.
If policy review and updating feels like a makimaki/monkey on your back, contact us now for help. You can schedule a free 30 minute consultation about your needs and your best policy solution. We can take care of the reviews and updating.
If you’re a DIY policy person, tick off these changes as you review your organisation’s policies and procedures.
Legislation changes
Key changes that have commenced this year have been:
- new provision for family violence leave and variation of employment terms for staff affected by family violence
- changes to the law relating to family violence including how and when family violence information can be shared between authorised services and persons
- changes relating to information-sharing for child protection and wellbeing purposes
- extension of Oranga Tamariki legislation (statutory care and youth justice) to under 18 years (was previously up to 17 years)
- more support for young people leaving statutory care or custody up to 25 years
- new principles to guide decisions and interventions under the Oranga Tamariki legislation (eg addressing mana tamaiti, recognition of whakapapa and involvement of those with whanaungatanga responsibilities)
- new requirements on the CE of Oranga Tamariki to enter strategic partnerships with iwi, to give practical effect to Te Tiriti o Waitangi and to report and monitor performance on outcomes for tamariki Māori
- the introduction of new care standards setting minimum requirements for the statutory care of tamariki.
Practice
And don’t forget relevant practice and sector developments that are important enough to incorporate into your policies and procedures, for example:
- stronger recognition across sectors of whānau-centric practice
- more recognition of the need for trauma-informed responses
- move from 3 Ps Treaty framework to article-based framework
- more focus on workplace health and wellbeing
- focus on cultural safety and cultural competency
- mainstreaming – equality and accessibility
- individualised funding.
Quit feeding the makimaki!
Usually, people contact us because they know their policies and procedures are not up to date. They are busy managing services like social housing, family violence intervention, care, mental health, counselling, perpetrator programmes, family support, sexual violence services etc.
They haven’t got the time to keep their organisations’ policies and procedures up-to-date. They no longer want the worry of it.
If this is you, contact us now. We can take care of your policy reviews and updating. Finally, you can get say “goodbye” to that makimaki on your back!
Learning from the Waitangi Tribunal Māori health report
The first report from the Waitangi Tribunal of its Kaupapa Inquiry into Māori health – Hauora – was released this month. It concluded that our primary health care system has failed to achieve Māori health equity; that New Zealand’s legislative, policy and administrative framework is not, in fact, fit to achieve this outcome.
News reports have highlighted the Tribunal’s findings of institutional racism. Here, we discuss some other aspects of the Tribunal’s report to help agencies give effect to some of the gems in the report (eg in their policies and practices).
We look first at the Tribunal’s approach to the Crown’s 3 Ps Treaty framework. We then look at new Treaty principles proposed by the Tribunal. Later, at some strategies for reflecting these principles.
The “3 Ps” – out with the old
The “3 Ps” comprise the well-established Crown Treaty framework – the principles of partnership, participation and protection. They came out of the Royal Commission on Social Policy in 1986.
The Tribunal described these principles as outdated and the Crown accepted that they reflect a “reductionist view” of the Treaty (Hauora, p79).
Thirty years on, with a lot more Treaty jurisprudence and Treaty settlements under our national belt, there’s clearly room to do better. The Tribunal proposes a new set of Treaty principles for New Zealand’s primary health care framework.
They are principles the Tribunal has relied on in a number of key reports (eg Te Whānau o Waipereira Report; The Napier Hospital and Health Services Report; Tū Mai Te Rangi! Report on the Crown and Disproportionate Reoffending Rates.) They are relevant to all sectors. We briefly outline them below by reference to the articles of Te Tiriti o Waitangi.
Tribunal treaty principles
Principle 1: Recognition and protection of tino rangatiratanga
This is guaranteed under Article 2 of Te Tiriti. It means that the right of Māori to organise in whatever way they choose – whānau, hapū, iwi or other form of organisation and to exercise autonomy and self-determination to the greatest extent must be recognised and protected.
Principle 2: Equity
This is an Article 3 Treaty commitment. It’s also about acting in good faith as a Treaty partner.
Equity is not just about allowing equal access to healthcare or other services for all. The Waitangi Tribunal highlighted that equity is also not just about reducing disparities. It involves the bigger goal of equitable outcomes for Māori.
The Tribunal approved the World Health Organisation’s definition “Equity is the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically.” (Hauora, p67)
Principle 3: Active protection
This principle is all about action and leadership. Devolution and permissive arrangements without Treaty leadership are not sufficient. Provision for equal opportunity or a “one-size fits all” approach also falls short.
The Crown must actively pursue and do whatever is reasonable and necessary to ensure the right to tino rangatiratanga and to achieve equitable health and social outcomes for Māori.
Principle 4: Partnership
Yes, this “P” remains. Its meaning reflects an interplay of articles 1 and 2 of Te Tiriti o Waitangi.
For the Crown to be a good governor it must recognise and respect the status and authority of Māori to be self-determining in relation to resources, people, language and culture (ie tino rangatiratanga). It must involve Māori at all levels of decision making.
Both the Treaty parties must act reasonably and in good faith towards each other.
Principle 5: Options
This principle is about giving real and practical effect to the principles of tino rangatiratanga and equity; articles 2 and 3 of Te Tiriti. Where kaupapa Māori services exist, Māori should have the option of accessing them as well as culturally appropriate mainstream services. They should not be disadvantaged by their choice.
It’s the job of the Crown to ensure each option is viable and sustainable by providing sufficient financial and logistical support, strong leadership and effective monitoring.
Report findings
The Tribunal concluded that the Crown had breached the Treaty in a number of ways. It found that from inception Māori primary health care organisations have been significantly underfunded, leading to a decline in the number of services. Whereas at a peak there were 14 Māori primary health organisations in the country, there are now only four (Hauora,p156).
A similar story of unrealised potential and breaches of the partnership and tino rangatiratanga obligations can undoubtedly be told in other sectors. For example, Iwi Social Services and Maatua Whangai were incorporated into the Childrens Young Persons and their Families Act (ie Oranga Tamariki Act) in 1989. They were established to play a key role in the statutory care system in response to Puao-Te-Ata-tu. However, they were undermined by a lack of resourcing and support (eg Shane Walker, Maatua Whangai o Otepoti Reflections -ANZASW).
The Tribunal report makes a number of recommendations. This includes two interim recommendations, that:
- an independent Māori statutory authority be explored
- the Crown and claimants work on a way of assessing the extent of underfunding of Māori primary health organisations and providers.
The parties must report back to the Tribunal on progress with these after 7 months.
Some learnings
There’s some great learning in the Tribunal report about giving effect to Te Tiriti o Waitangi. Some key points for organisations’ policies and practice are that:
- agencies should have a strong leadership focus on fulfilling Treaty obligations and achieving equitable outcomes for Māori
- feedback and data should be gathered about access and outcomes for Māori. It should be regularly reviewed, evaluated and used to support continuous improvement
- if you’re not making progress be wary of attributing blame to clients. Instead, consider different ways of delivering your service
- avoid deficit language “hard to reach”, “vulnerable children” that tend to individualise what are often structural or system issues
- consider and invest time, good faith and energy into building constructive treaty partnerships (with mana whenua, local Māori, tau iwi agencies)
- the Crown must ensure funding of kaupapa Māori services is sufficient for their viability and that mainstream services it funds are competent to provide services to Māori (ie staff and board are culturally competent)
- Māori are engaged at all levels of social and health sector decision-making from governance through to service delivery.
More to come
There’s more in this and other Waitangi Tribunal reports to learn from. Like other Tribunal reports its rich in opportunities to learn about Treaty compliance.
In another blog we’ll take a look at how the Social Sector Accreditation Standards- Level 2 and Core Health and Disability Standards line up with the Tribunal’s approach.
Get in touch with us if you’re wanting help with your policies and procedures. We love to hear from you.